Introduction
Physiotherapy in Kitchener for Knee
Welcome to Kitchener Physiotherapy & Wellness patient resource about Revision Arthroplasty of the Knee.
Over the past 30 years, artificial knee replacement surgery has become increasingly common. Millions of people have gotten a new knee joint. The first time a joint is replaced with an artificial joint the operation is called a primary joint replacement. As people live longer and more people receive artificial joints, some of those joints begin to wear out and fail. When an artificial knee joint fails, a second operation is required to replace the failing joint. This procedure is called a revision arthroplasty.
This article will help you understand:
- why revision surgery becomes necessary
- what happens during the operation
- what to expect during your recovery
Related Document: Kitchener Physiotherapy & Wellness's Guide to Artificial Joint Replacement of the Knee
Anatomy
What part of the knee is affected?
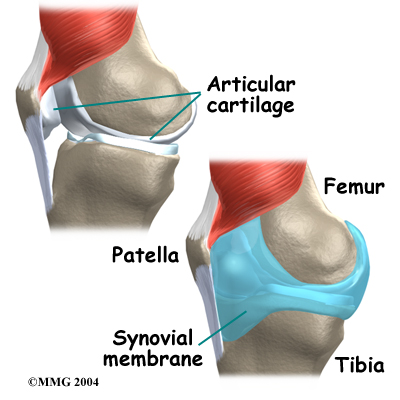
The knee joint is formed where the thighbone (femur) meets the shinbone (tibia). A slick cushion of articular cartilage covers the ends of both of these bones so that they slide against one another smoothly. The articular cartilage is kept slippery by joint fluid made by the joint lining (synovial membrane). The fluid is contained in a soft tissue enclosure around the knee joint called the joint capsule.
The kneecap (patella) is the moveable bone on the front of the knee. It is wrapped inside a tendon that connects the large muscles on the front of the thigh (the quadriceps muscles) to the tibia. The back of the patella is covered
with articular cartilage. The patella glides within a groove on the front of the femur.
Related Document: Kitchener Physiotherapy & Wellness Guide to Knee Anatomy
Knee Anatomy Introduction
Rationale
Why does a knee revision become necessary?
The most common reasons for knee revision arthroplasty are:
- mechanical loosening
- infection in the joint
- fracture of the bone around the joint
- instability of the implant
- wear of one or more parts of the implant
- breakage of the implant
Mechanical Loosening
Mechanical loosening means that for some reason (other than infection) the attachment between the artificial joint and the bone has become loose. There are many reasons why this can occur. It may be that, given enough time, all artificial joints will eventually loosen. This is one reason that surgeons like to wait until absolutely necessary to put in an artificial joint. The younger you are when an artificial joint is put in, the more likely it is that the joint will loosen and require a revision. Mechanical loosening can occur in both cemented and uncemented artificial joints. (The different types of joints are described later.)
Infection
If an artificial joint is infected, it may become stiff and painful. It may also begin to lose its attachment to the bone. An infected artificial joint will probably have to be revised to try to cure the infection.
In the knee joint, operations to exchange the original implant (prosthesis) with a new one have a good chance of success. The decision to do a revision surgery depends in part on the type of bacteria that has infected the joint. In some uncommon cases, the type of bacteria is so harmful that a revision is not possible. In these unfortunate cases, the surgeon may suggest placing a cement spacer filled with antibiotics in the knee and having the patient wear a knee brace for support. In rare cases, the knee may need to be fused together, or possibly even amputated. In less aggressive infections, the infected artificial joint is removed at one operation. Antibiotics are given for up to three months until the infection is gone. Then a second operation is done to insert a new artificial knee.
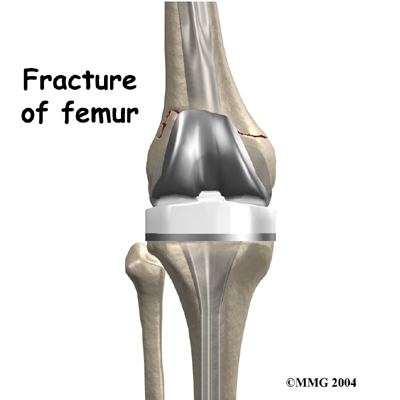 Fracture
Fracture
A fracture may occur near an artificial joint. It is sometimes necessary to use a new artificial joint to fix the fracture. For example, if the where the prosthesis attaches, it may be easier to replace the femoral part of the artificial joint with a new piece that has a longer stem that can hold the fracture together while it heals.
This is similar to fixing the fracture with a metal rod.
Instability
Instability means that the artificial joint dislocates. This is very painful when it happens.
It is unlikely that the knee joint will completely dislocate. However, it can happen. It is more common for the knee joint to be either too tight or too loose.
If the knee joint is too loose, it can cause unsteadiness and pain. If the joint is too tight, the knee is usually painful and doesn't have a good range of motion.
Wear
With the rise in knee joint replacements, surgeons have begun to see wear in the plastic parts of the artificial joints. In some cases, if the wear is discovered in time, the revision may only require changing the plastic part of the artificial joint. If the wear continues until the metal is rubbing on metal, the whole joint may need to be replaced.
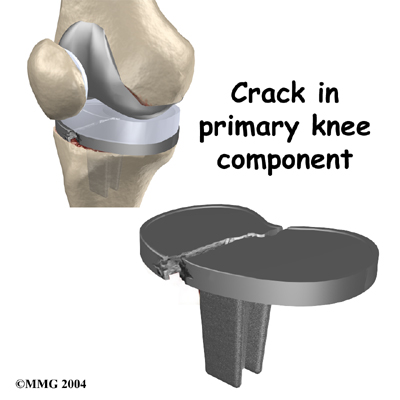
Breakage
Finally, the metal of the artificial joint can due to the constant stress that the artificial joint undergoes everyday. In weight-bearing joints like the knee, this is greatly affected by how much you weigh and how active you are.
Preparation
What happens before surgery?
Your surgeon will carefully plan the revision operation. Before the operation, many possible options and complications will have to be taken into account. Your surgeon will discuss these with you. Be sure to ask if there are parts of the procedure, your recovery, or the risks associated with a revision joint replacement that you have questions about.
Once the decision to proceed with surgery is made, several things may need to be done. Your orthopedic surgeon may suggest a complete physical examination by your medical or family doctor. This is to ensure that you are in the best possible condition to undergo the operation.
You may be scheduled for a bone scan so the surgeon can check for loosening of the artificial joint. When an artificial joint is loose, the bone around the joint reacts by trying to form new bone, a process called remodeling. The bone scan is done by injecting you with a weak radioactive chemical. Several hours later, a large camera is used to take a picture of the bone around the artificial joint. If the artificial joint is loose and there is remodeling going on, the picture will show a hot spot where the chemical has been added to the newly forming bone. The brighter the hot spot, the more likely it is that the artificial joint is loose.
 If your surgeon suspects that the artificial knee is loose, other tests may be necessary to find out why the joint is loose. Before any plans are made to revise the artificial joint, most orthopedic surgeons will want to make sure that the knee is not loose because of infection. To check for infection, blood tests may be ordered. Your surgeon may also need to your knee. This involves inserting a needle into your knee joint, removing fluid, and sending the contents to the laboratory. Replacing any artificial joint that is infected is much more involved than replacing a noninfected, loose artificial joint. In some cases, infection will make a revision impossible.
If your surgeon suspects that the artificial knee is loose, other tests may be necessary to find out why the joint is loose. Before any plans are made to revise the artificial joint, most orthopedic surgeons will want to make sure that the knee is not loose because of infection. To check for infection, blood tests may be ordered. Your surgeon may also need to your knee. This involves inserting a needle into your knee joint, removing fluid, and sending the contents to the laboratory. Replacing any artificial joint that is infected is much more involved than replacing a noninfected, loose artificial joint. In some cases, infection will make a revision impossible.
Skin problems are common for people having knee revision arthroplasty. People who have low levels of lymphocytes (white blood cells that form antibodies to fight off infection) have an even greater risk of incision problems. Your surgeon may request a blood count before surgery to make sure you have adequate numbers of lymphocytes.
Past incisions in the knee can further complicate the planned revision procedure. People needing a knee revision will have at least one previous knee incision. Most surgeons who do knee revision surgery prefer to make an incision that runs down the center of the knee. This may not be possible due to previous knee incisions. The second choice is usually toward the outer (lateral) side of the knee. (Lateral is the side furthest from your other knee.) If the skin appears to be too tight for a planned incision to close, the risk of wound complications is high after the revision procedure. The orthopedic surgeon may need to consult with a plastic surgeon to ensure the best approach and result.
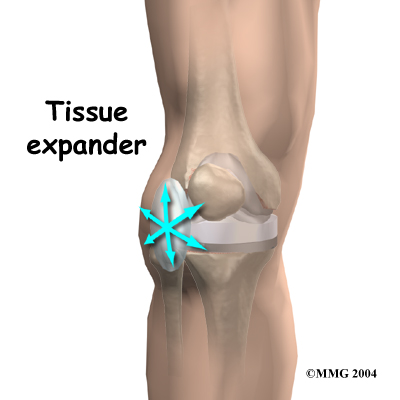 Another option is to use . These are placed just under the skin next to where the revision incision will eventually go. The expanders stay in for up to eight weeks and are removed when you go in for the revision surgery. The idea is that the skin will have stretched enough so that, when the revision procedure is done, the edges of the skin can be closed and sutured together.
Another option is to use . These are placed just under the skin next to where the revision incision will eventually go. The expanders stay in for up to eight weeks and are removed when you go in for the revision surgery. The idea is that the skin will have stretched enough so that, when the revision procedure is done, the edges of the skin can be closed and sutured together.
Before surgery, you may also need to spend time with the physiotherapist who will manage your rehabilitation after the surgery. The physiotherapist begins the teaching process before surgery to ensure that you are ready for rehabilitation afterwards. One purpose of the preoperative therapy visit is to record a baseline of information. This includes measurements of your current pain levels, functional abilities, and the available movement and strength of each knee. Any swelling in the artificial knee is noted.
A second purpose of the preoperative physiotherapy visit is to prepare you for your upcoming surgery. You will begin to practice some of the exercises you will use just after surgery. You will also be trained in the use of either a walker or crutches. Finally, an assessment will be made of any needs you will have at home once you're released from the hospital.
You may be asked to donate some of your own blood before the operation. This blood can be donated three to five weeks earlier. Your body will make new blood cells to replace the loss. If you need a blood transfusion during the operation, you will receive your own blood back from the blood bank.
Surgical Procedure
What happens during the operation?
Before describing the revision procedure, let's look at the revision prosthesis itself.
The Revision Prosthesis
There are two major types of revision implants:
- cemented prosthesis
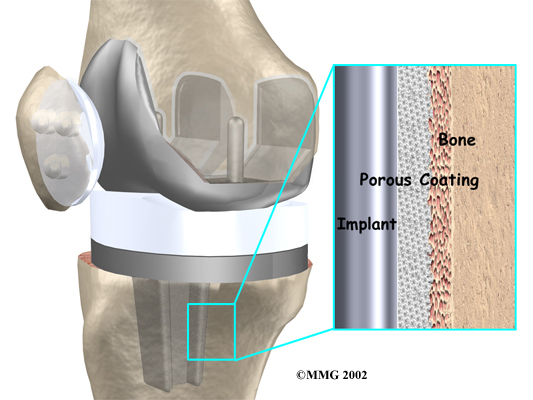
- uncemented prosthesis
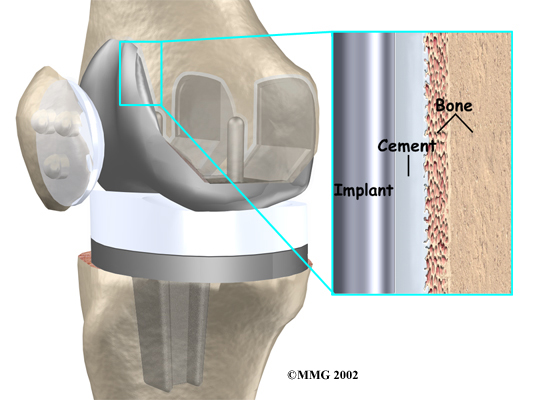
A is held in place by a type of epoxy cement that attaches the metal to the bone. An has a fine mesh of holes on the surface that allows bone to grow into the mesh and attach the prosthesis to the bone.
Both are still widely used. In many cases a combination of the two types is used. The patellar (kneecap) portion of the prosthesis is commonly cemented into place. The decision to use a cemented or uncemented artificial knee is usually made by the surgeon based on your age, your lifestyle, and the surgeon's experience.
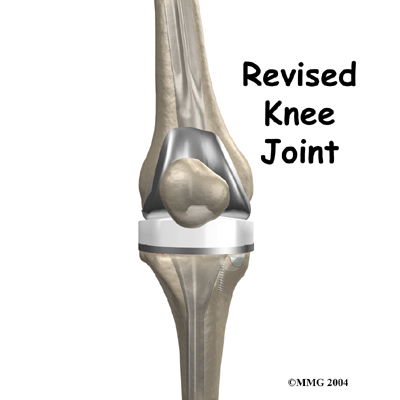
Each prosthesis is made up of three main parts.
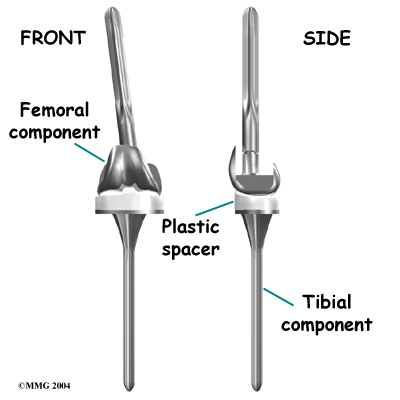
The tibial component (bottom portion) replaces the top surface of the lower bone, the tibia. The stem of the tibial component used in revision surgery is usually much longer than the type used for primary knee replacements. This is because the bone of the tibia is usually not the same as when the initial replacement was done. The bone may be weaker, or there may be areas inside the tibia where bone is missing. A longer stem can reach further down the tibial canal and distribute your body weight better. It also gives the body a greater surface area for healing, which can improve fixation of the implant to the bone inside the tibia.
The femoral component (top portion) replaces the bottom surface of the upper bone (the femur) and the groove where the patella fits. Like the tibial component used in revision, the femoral component often has a long stem.
The patellar component (kneecap portion) replaces the surface of the patella where it glides in the groove on the femur.
The tibial component is usually made of two parts: a metal tray that is attached directly to the bone, and a plastic spacer that provides the slick surface. The femoral component is made of metal. In some types of knee implants, the patellar component is made of a combination of metal and plastic.
The Operation
To begin the procedure, the surgeon makes an incision down the front of the knee to allow access to the joint. The surgeon attempts to open the knee joint with the least amount of damage to the muscles and ligaments around the joint.
Next, the original artifical joint is removed. When the primary artificial joint was put in with cement, the cement has to be removed from inside the canal of the femur and the tibia. Because the bone is often fragile and the cement is hard, removing the cement can cause the femur or tibia to fracture during the operation. This is not unusual, and in most cases the surgeon will simply continue with the operation and fix the fracture as well.
Samples of bone and marrow tissue are usually removed during the surgery and sent to a laboratory to see if any infection is present. If an infection is present, a new artificial joint will probably not be put in (see below).
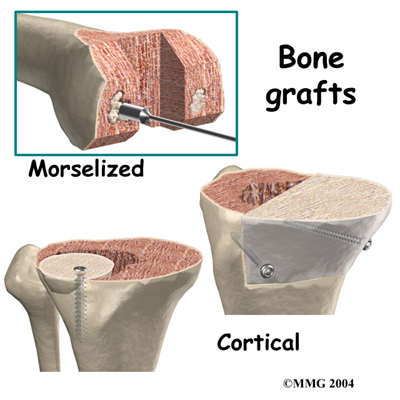 Revision joint replacements are much different from primary joint replacements. One reason that revision procedures are not routine is that there is almost always bone loss around the primary prosthesis. The surgeon deals with this problem by placing a or some other material around the artificial joint to reinforce the bone. This bone graft may come from your own body, such as bone taken from the pelvis during the same operation. This type of graft is called an autograft.
Revision joint replacements are much different from primary joint replacements. One reason that revision procedures are not routine is that there is almost always bone loss around the primary prosthesis. The surgeon deals with this problem by placing a or some other material around the artificial joint to reinforce the bone. This bone graft may come from your own body, such as bone taken from the pelvis during the same operation. This type of graft is called an autograft.
If the amount of bone needed is too large to take from your body, your surgeon may choose to use bone graft from the bone bank. This type of bone graft has been taken from someone else and placed in the bone bank. This type of transplant is called an allograft.
After application of bone and other materials to rebuild the tibia and/or femur, a new prosthesis is implanted. It is challenging to imitate the natural shape of the bones after rebuilding the bone, so a specially designed prosthesis is usually needed. All of this is carefully planned by the surgeon before the operation.
To get the best and sturdiest fit between the tibial and femoral components, the surgeon adjusts and balances the soft tissues that surround the knee joint. This may require cutting or tightening the ligaments on each side of the knee. Afterward, the surgeon checks the fit of the new knee components with the knee bent and then with the knee straightened. Further adjustment is made by changing out a thicker plastic portion of the tibial component. In the end, the surgeon tries to get the best fit so that the knee is stable through a full range of movement.
When the tibial and femoral components are in place and the soft tissues have been balanced, the surgeon will address the patella. In some cases, the patella may not need to be revised, especially when the surgeon sees good fixation of the original patellar implant. Sometimes the old patella component is simply removed, allowing the bone on the back of the patella to glide against the smooth surface on the front of the revision femoral component. In either case, the surgeon checks to see that the patella is lined up correctly and that it rides normally within the groove in the front of the femur.
Finally, the soft tissues of the knee are sewn back together, and metal staples or stitches are used to hold the skin incision together.
A revision joint replacement of the knee is more complex and unpredictable than a primary joint replacement. Since many factors can influence its longevity, your surgeon will not be able to say exactly how long your revision will last. Also, keep in mind that because revision surgery is more complicated than primary joint replacement, it may take up to a year to be able to perform your routine daily activities. Often people continue to need a walking aid because knee pain increases when they are on their feet for prolonged periods. There is also a greater chance that the knee will be tight and unable to bend all the way after knee revision surgery.
In some cases, if an artificial joint fails, it may not be possible to put another artificial joint back in. This can occur if the primary joint has failed because of an infection that cannot be controlled, if the bone has been destroyed so much that it will not support an artificial joint, or if your medical condition will not tolerate a major operation.
Sometimes a choice other than knee revision is best because a big operation might result in a failure, or even death. Removing the prosthesis and not replacing it doesn't mean the patient can't walk anymore. The surgeon may suggest fusing the joints of the knee, placing a spacer in the joint, or in some cases amputating the leg.
Complications
What might go wrong?
As with all major surgical procedures, complications can occur. This document doesn't provide a complete list of the possible complications, but it does highlight some of the most common problems. Some of the most common complications following revision arthroplasty of the knee include:
- anesthesia complications
- thrombophlebitis
- infection
- myositis ossificans
- loosening
- incision complications
Anesthesia Complications
Most surgical procedures require that some type of anesthesia be done before surgery. A very small number of patients have problems with anesthesia. These problems can be reactions to the drugs used, problems related to other medical complications, and problems due to the anesthesia. Be sure to discuss the risks and your concerns with your anesthesiologist.
Thrombophlebitis (Blood Clots)
Thrombophlebitis, sometimes called deep venous thrombosis (DVT), can occur after any operation, but it is more likely to occur following surgery on the hip, pelvis, or knee. DVT occurs when the blood in the large veins of the leg forms blood clots. This may cause the leg to swell and become warm to the touch and painful. If the blood clots in the veins break apart, they can travel to the lung, where they lodge in the capillaries and cut off the blood supply to a portion of the lung. This is called a pulmonary embolism. (Pulmonary means lung, and embolism refers to a fragment of something traveling through the vascular system.) Most surgeons take preventing DVT very seriously. There are many ways to reduce the risk of DVT, but probably the most effective is getting you moving as soon as possible. Two other commonly used preventative measures include:
- pressure stockings to keep the blood in the legs moving
- medications that thin the blood and prevent blood clots from forming
Infection
Infection can be a very serious complication following an artificial joint revision. Some infections may show up very early, even before you leave the hospital. Others may not become apparent for months, or even years, after the operation. Infection can spread into the artificial joint from other infected areas. Your surgeon may want to make sure that you take antibiotics when you have dental work or surgical procedures on your bladder and colon to reduce the risk of spreading germs to the joint.
The risk of infection is higher in revision arthroplasty than in primary joint replacement. In a primary knee replacement, the risk of infection is less than one percent. It goes up to two percent or more in revision cases. These figures are only an estimate and vary between different scientific studies.
Myositis Ossificans
Myositis ossificans is a curious problem that can affect the knee after both a primary knee replacement and a revision knee replacement. The condition occurs when the soft tissue around the knee joint begins to develop calcium deposits. Myositis means inflammation of muscle, and ossificans refers to the formation of bone. This can lead to a situation where new bone actually forms along the sides and top of the knee. This leads to stiffness and a loss of motion in the knee joint. It also causes pain.
Myositis ossificans is more common in people who have a long history of osteoarthritis with multiple bones spurs. Something about the genetic makeup in these people makes them more likely to produce bone tissue. Major reconstruction operations such as a knee revision seem to do more damage to the surrounding tissues than primary knee replacements. The operation is simply longer and harder to do. Calcium deposits are also more likely to form.
The treatment of myositis ossificans may actually begin before you get it. In cases where you are at high risk for developing this condition, your surgeon may recommend that you take medications such as indomethacin after surgery. This medication reduces the tendency for bone to form and may protect you from developing myositis ossificans.
A much more effective method that has been used a great deal to prevent the development of myositis ossificans involves radiation treatments immediately after surgery. These are the same type of radiation treatments used to treat cancer. Several short radiation treatments begun the day after surgery and continued for three to five days seem to drastically reduce the risk of developing myositis ossificans.
If myositis ossificans forms despite these precautions, treatment will depend on how much it affects your knee. Your surgeon will note how much pain it causes and how much it restricts motion. In some severe cases, you may choose to have a second operation to remove the calcified tissue that has formed. This is usually followed by radiation treatments to prevent the calcium deposits from returning.
Loosening
The major reason that artificial joints eventually fail continues to be from loosening where the metal or cement meets the bone. A loose revised prosthesis is a problem because it causes pain. Once the pain becomes unbearable, another revision surgery may be needed. The rate of loosening is higher after revision surgery than in primary arthroplasties.
Incision Complications
Poor healing of the incision is a fairly common complication of knee revision arthoplasty. This is because the tissue is often scarred and thinner than when the original knee replacement was done. The blood supply to the skin may not be normal due to damage to the blood vessels from one or more previous knee surgeries. As mentioned earlier, previous skin incisions can make it hard for the incision to close after knee revision surgery, leading to complications. When the incision doesn't heal right, the chances of infection go up. The wound may continue to ooze, creating optimal conditions for bacterial growth.
Poor incision healing is more likely to occur in patients with one or more of the following factors:
- anemia
- obesity
- past wound healing problems
- weak immune system
- tobacco habit
- poor circulation
- diabetes mellitus
Your surgeon's goal is to prevent problems with the incision. If problems do happen, however, one or more additional surgeries will likely be needed.
After Surgery
What happens after surgery?
After surgery, your knee is covered with a padded dressing. Special boots or stockings are placed on your feet to help prevent blood clots from forming.
If a general anesthesia was used, a nurse, physiotherapist, or respiratory therapist will visit your room to guide you in a series of breathing exercises. You'll use an incentive spirometer to improve breathing and avoid possible problems with pneumonia.
Several measures may be taken for patients who are at risk of incision problems. Some surgeons believe it is important to place a drain in the knee for a few days after surgery. The idea is that the drain will help keep swelling down. Too much swelling can pull the new incision apart and allow the wound to ooze. These factors place the knee at risk for infection. The practice of putting a drain in the knee is controversial, however, as some surgeons think that implanting the drain carries by itself an even bigger risk of infection.
A second measure to improve wound healing is to supply extra oxygen for three to four days through a nasal cannula. (A nasal cannula delivers oxygen through two small prongs placed into the nose.) The idea is that the added oxygen circulating in the blood stream will speed up the healing process and reduce the risk of incision problems.
You may also have physiotherapy treatments once or twice each day as long as you are in the hospital. Therapy treatments will address the range of motion in the knee. Your therapist may also demonstrate exercises to improve knee mobility and engage the thigh and hip muscles. Ankle movements help pump swelling out of the leg and prevent the possibility of a blood clot.
When you are stabilized, your physiotherapist will help you up for a short outing using your crutches or walker. After surgery, you may not be allowed to put weight on the affected leg for a period of time. This varies from surgeon to surgeon.
Most patients are able to go home after spending four to seven days in the hospital. You'll be on your way home when you can get in and out of bed, walk up to 75 feet with your crutches or walker, go up and down stairs safely, and access the bathroom. It is also important that you regain a good muscle contraction of the quadriceps muscle and that you gain improved knee range of motion. Patients who need extra care may be sent to a different unit of the hospital until they are safe and ready to go home.
Most orthopedic surgeons recommend that you have routine checkups after your revision surgery. How often you need to be seen varies from every six months to every five years, according to your situation and what your surgeon recommends. You should always consult your orthopedic surgeon if you begin to have pain in your artificial joint or if you begin to suspect something is not working correctly.
Kitchener Physiotherapy & Wellness provides services for physiotherapy in Kitchener.
Portions of this document copyright MMG, LLC.
Our Rehabilitation
What should I expect during my recovery?
Your staples will be removed about two weeks after surgery. Patients are usually able to drive within eight weeks and walk without a walking aid by two to three months. Upon the approval of our therapist, patients are generally able to resume sexual activity by six to eight weeks after surgery.
When you begin your Kitchener Physiotherapy & Wellness rehabilitation, our physiotherapist may first use heat, ice, or electrical stimulation if you are still having swelling or pain. During this time, you should continue to use your walker or crutches as instructed. If you had a cemented procedure, you'll advance the weight you place on your sore leg as much as you feel comfortable. If you had a noncemented procedure, place only the toes down until you've had a follow-up X-ray and our physiotherapist directs you to put more weight through your leg (usually by the fifth or sixth week after surgery). Although recovery time varies, most patients progress to using a cane in six to eight weeks.
Our physiotherapist may use hands-on stretches for improving your range of motion, then strength exercises to address key muscle groups including the buttock, hip, thigh, and calf muscles. Endurance can be improved through stationary biking, lap swimming, and using an upper body ergometer (upper cycle).
Our physiotherapists sometimes treat patients in a pool. Exercising in a swimming pool puts less stress on the knee joint, and the buoyancy lets you move and exercise easier. Once you've gotten your pool exercises down and the other parts of your rehab program advance, our physiotherapist
may instruct you in an independent program.
When you are safe in putting full weight through the leg, our physiotherapist will choose several types of balance exercises to further stabilize and control the knee. Finally, we will use a select group of exercises to simulate day-to-day activities, such as going up and down steps, squatting, and walking on uneven terrain. Other specific exercises may then be chosen to simulate work or hobby demands.
Our physiotherapist will work with you to help keep your revised knee joint healthy for as long as possible. This may require that you adjust your activity choices to keep from putting too much strain on your revised knee joint. Heavy sports that require running, jumping, quick stopping and starting, and cutting are discouraged. Patients may need to consider alternate jobs to avoid work activities that require heavy lifting, crawling, and climbing.
At Kitchener Physiotherapy & Wellness, our goal is to help you maximize strength, walk normally, and improve your ability to do your activities. When your recovery is well under way, regular visits to our office will end. Although we will continue to be a resource, you will be in charge of doing your exercises as part of an ongoing home program.
Kitchener Physiotherapy & Wellness provides services for physiotherapy in Kitchener.
Portions of this document copyright MMG, LLC.